
Right Track? Nation’s Worst? What’s the Diff?
Posted: May 2, 2014 Filed under: Healthcare, Policy Leave a comment Tennessee state house speaker Beth Harwell picked an odd week to write an op-ed (in this morning’s Tennessean) declaring that “Tennessee is on the right track” — unless she equates “on the right track” with “among the nation’s worst.” Because “among the nation’s worst” is precisely and appropriately how Tennessean reporter Shelley DuBois sums up the state’s standing in a new Commonwealth Fund report comparing states on dozens of measures of health care access, quality, costs and outcomes.
Tennessee state house speaker Beth Harwell picked an odd week to write an op-ed (in this morning’s Tennessean) declaring that “Tennessee is on the right track” — unless she equates “on the right track” with “among the nation’s worst.” Because “among the nation’s worst” is precisely and appropriately how Tennessean reporter Shelley DuBois sums up the state’s standing in a new Commonwealth Fund report comparing states on dozens of measures of health care access, quality, costs and outcomes.
The report titled Aiming Higher (full text pdf here), which covers the period 2007-2012, finds widespread gains among states in areas that were getting a lot of policy attention, such as child immunizations and hospital readmissions, but on the down side rising costs and declines in access to care. In comparisons of states, Tennessee comes out rather badly. Skimming through the report’s various charts and graphs (pdf), this is easy to see.
Exhibit 12: Percent of adults who went without care because of cost, Tennessee ranks 10th from the bottom, unchanged from 2007.
Exhibit 16: Mortality amenable to heath care, Tennessee is in the bottom 10 for both black and white residents (they do that one by race).
Exhibit 8: Tennessee has the 16th highest rate of Medicare 30-day readmissions.
Exhibit 3: An overall state scorecard summary of health system performance across five dimensions (access and affordability; prevention and treatment; avoidable hospital use and cost; health lives; equity) ranks Tennessee’s 40th, in the bottom quartile.
Two bright spots: Exhibit 6 shows Tennessee ranks 11th in percent of children receiving all recommended vaccine doses, and Exhibit 11 shows Tennessee in top third of states in percent of children with insurance.
Perhaps these weak results mask improvement, making it possible to couch them in Harwell’s “on the right track” optimism. Is that plausible? Not so much. The CF report captures trends in Tennessee on 34 indicators, and finds improvement on 12 of them, worsening on 10, and no change on the rest — pretty much a wash. With the state’s ongoing stubborn refusal to entertain Medicaid expansion, it’s hard to look at the data here and predict upward movement in Tennessee’s health care quality and outcomes anytime soon.
“Right track” indeed.
A version of this post appears on the Nashville Scene‘s Pith in the Wind blog.
My Last Marsha Post. Promise.
Posted: November 1, 2013 Filed under: Healthcare, Politics Leave a comment
“I demand to be taken seriously.”
Asserting that “some people like to drive a Ford and not a Ferrari, and some people like to drink out of a red solo cup and not a crystal stem,” Blackburn argued that people should be free to keep the cut rate insurance they have rather than be compelled to buy some of that highfallutin’ Marxist-Leninist Obamacare coverage. Sally Kohn at Salon captures it well, summing up Blackburn’s argument as a brief for the principle that “Americans should be free to hold onto their inadequate, costly and reckless insurance policies that throw them off at the slightest sign of illness while forcing costs up for the rest of us.”
Without question, this is to a significant extent a self-inflicted wound at the White House, which willfully enabled this latest tactical conservative assault on the Affordable Care Act through Obama’s repeated assertions going back three years that under ACA people could keep their existing health insurance if they wished. Although NBC News would have us be stunned by the revelation that the Obama administration knew this claim to be exaggerated, it was actually pretty obvious to anyone paying attention from the outset that ACA would compel many to encounter significant changes in health insurance coverage. A lot of us were cringing at Obama’s repeated assertions on this when he first started making them.
But that doesn’t impeach the imbecility of Blackburn’s way of “thinking” — that no health insurance policy exists that is too flimsy to meet the needs of her fine constituents. Look, she has every right to believe that health insurance should be a wholly unregulated market, but she needs to make the case for that, not just rail against regulatory standards merely because they are regulatory standards. Would she do away with all regulation of all insurance? Does she have even a clue as to the implications of doing so? If you want to use your Congressional perch to shout down administration officials with nostrums of free market liberatarian orthodoxy, it might behoove you and your staff to spent at least a few minutes understanding how these markets and regulatory schemes work, and what the actual policy consequences of doing away with them might look like.
Ok, for real this time: No more Marsha posts.
A version of this post appears on the Nashville Scene‘s Pith in the Wind blog.
A City’s Competitive Edge: Cheap Colonoscopies!
Posted: June 3, 2013 Filed under: Healthcare Leave a comment A New York Times piece Sunday on the absurdly high price of health care in the U.S. compared to other countries zeroed in on everyone’s favorite medical intervention — the colonoscopy — as a particularly compelling example. We learn in the piece that colonoscopies cost a lot more in the U.S. than in other developed nations, but we also learn that the cost varies widely within the U.S.
A New York Times piece Sunday on the absurdly high price of health care in the U.S. compared to other countries zeroed in on everyone’s favorite medical intervention — the colonoscopy — as a particularly compelling example. We learn in the piece that colonoscopies cost a lot more in the U.S. than in other developed nations, but we also learn that the cost varies widely within the U.S.
Nashville, it turns out, is clearly a destination of choice for the price-conscious colonoscopy chopper. An analysis by Healthcare Blue Book looking at the highest amount paid for the procedure shows Nashville among the lowest of various metropolitan areas examined. Compared to our number, the upper bound price is more than double in Atlanta, Chicago and Denver, and more than triple in Austin. Only Baltimore is lower, and while they do also overachieve as a city in the all-important crab cake category, let’s face it … who really wants to live in Baltimore?
The map tells the story:
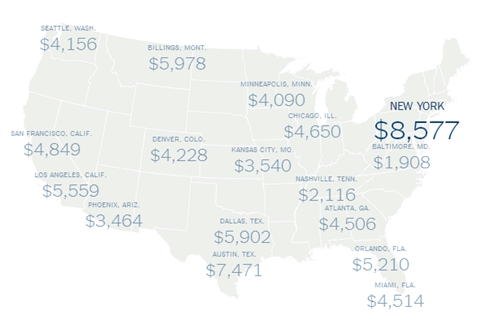
Each number is the highest amount paid for a colonoscopy in that metropolitan area.
Source: The New York Times
Finally, something Nashville does better than Austin! But can we leverage this competitive advantage? Colonoscopy tourism!
A version of this post appears on the Nashville Scene‘s Pith in the Wind blog.
Supremes on Medicaid: “Loaded Gun”?
Posted: July 3, 2012 Filed under: Healthcare, Policy Leave a comment
Although the insurance mandate gets most of the attention, many believe that it’s the Supreme Court outcome on Medicaid expansion within ACA that could have the longest lasting impact. Stanford professor Pamela Karlan wrote in last Sunday’s Times that the Roberts court ruling on Medicaid contributes to a neutering of federal power that should have liberals worrying big time:
For the first time since the New Deal, the court struck down an exercise of Congress’s spending power. It held that Congress lacked the power to deny Medicaid funds to states that refuse to expand their coverage. Chief Justice Roberts — joined by the liberal justices Stephen G. Breyer and Elena Kagan — held that while the government can deny additional Medicaid funds to states that refuse to expand their coverage, it cannot penalize them by rescinding current Medicaid payments. This is a loaded gun indeed.
Prof. Karlan notes that this is just the latest in a string of rulings curbing federal power, with cases coming down the pike next term on voting rights, affirmative action, same-sex marriage, and environmental affairs giving the Court opportunities to chip away further.
Without discounting Prof. Karlan’s conclusion that the trend at the Court gives “Americans who care about economic and social justice a reason to worry,” I do think after reading the Roberts opinion and the Ginsburg dissent carefully that she overstates a bit the ruling’s logic and argument on Medicaid (though granted, not the effect!). The Court held that the federal government can penalize states by rescinding current payments if the expansion is modest and incremental rather than radical. There is a fundamental difference of opinion between Roberts and Ginsburg over whether this particular expansion is modest or radical. To use the language in their back and forth in their opinions, is it a difference in kind (Roberts) or degree (Ginsburg)? Personally I’m inclined to side with Ginsburg and Sotomayor on this point, though it isn’t necessarily a simple or straightforward call.
It’s fascinating that this aspect of the case split the liberal wing of the Court — with Kagan and Breyer joining Roberts to find that it’s a difference in kind, not degree, and accordingly conclude that its overly coercive on the states. Perhaps they genuinely bought the Roberts formulation that the Medicaid expansion really is a difference in kind. But I am guessing that what tilted them might have been Roberts’ willingness to keep the ruling narrow — to say that the finding of undue coercion on the states invalidates only the threat to revoke all Medicaid funding to a state that rejects the new funding and conditions, but doesn’t (as the Scalia/Kennedy/Alito/Thomas cabal would have) invalidate the whole kit-n-kaboodle. Of course, Ginsburg and Sotomayor expressly at the end of their dissent bought into that limiting principle regarding what gets invalidated, making it possible for that narrow effect to prevail (otherwise the whole thing would could have been tossed). The coalition dynamics on the Court were fascinating on the Medicaid issue, arguably moreso than on the mandate.
A conspiracy theorist might argue that Roberts sold his conservative brethren out on the mandate in order to buy Breyer and Kagan’s support on the Medicaid aspect, getting what he really wanted most of all — Prof. Karlan’s loaded gun: the potentially huge dent in federal spending power that some construe in the Medicaid outcome. Hard to say, though, because these kinds of SCOTUS “turns” take a decade or two to really see in full.



